Adaptive Leadership
Adaptive leadership is a body of work, an area of study, and a practice concerned with how people make progress on problems that do not have clear definitions or known solutions.
These are the problems that matter most in health systems. They sit at the intersection of values, identity, power, loss, and responsibility. They persist despite expertise. They resist policy fixes. They generate heat, conflict, and fatigue precisely because what is required cannot be supplied by authority alone.
Adaptive leadership offers a way of understanding this kind of work, and of practicing it deliberately.
Exercising Leadership
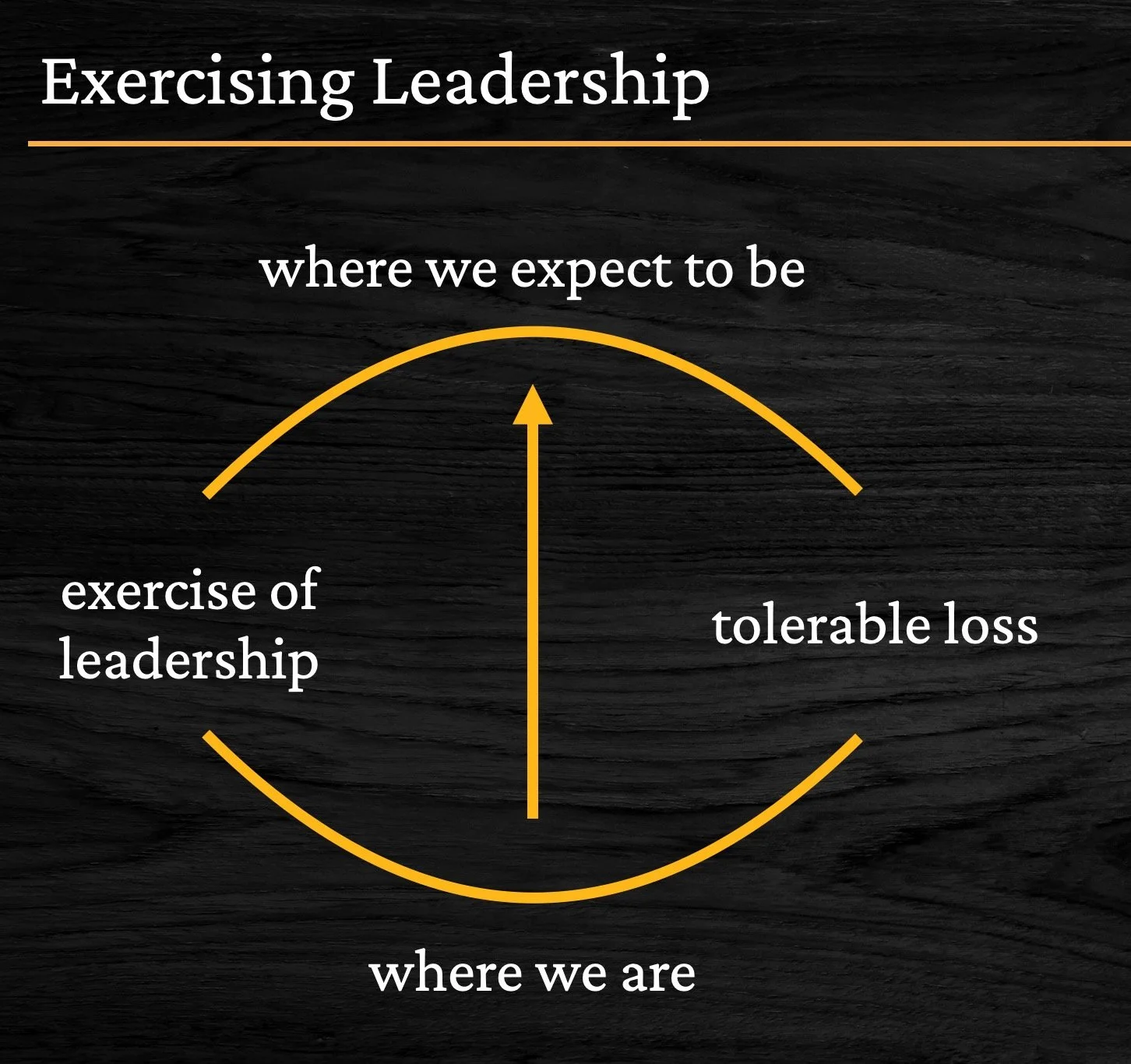
One of the central ideas in adaptive leadership is the distinction between where we are and where we hope to be, and the work required to move between the two.
That movement is rarely linear. It requires learning. It involves loss. It asks people to give up parts of what feels familiar, competent, or stabilizing in order to make room for something new.
Exercising leadership is the activity of mobilizing people to do that work.
This is not a description of a person or a role. It is a description of what is happening in the system.
Three kinds of problems
Adaptive leadership distinguishes between different kinds of challenges, because confusing them creates unnecessary failure.
Technical problems are well defined. Solutions are known. Expertise can be applied. If you have the right knowledge, resources, and authority, the problem can be solved.
Complicated problems may be difficult, but they are still largely technical. They require coordination, sequencing, and multiple forms of expertise. With enough time and effort, they can be worked through.
Adaptive problems are different. The problem itself is not fully agreed upon. Stakeholders hold competing values. Solutions require learning, shifts in behavior, and renegotiation of loyalties. Progress demands loss, and loss generates resistance.
Most health system challenges are mixtures of all three. Adaptive leadership is the practice of diagnosing which kind of work is actually required, and resisting the pull to apply technical solutions to adaptive problems.
Leadership and authority
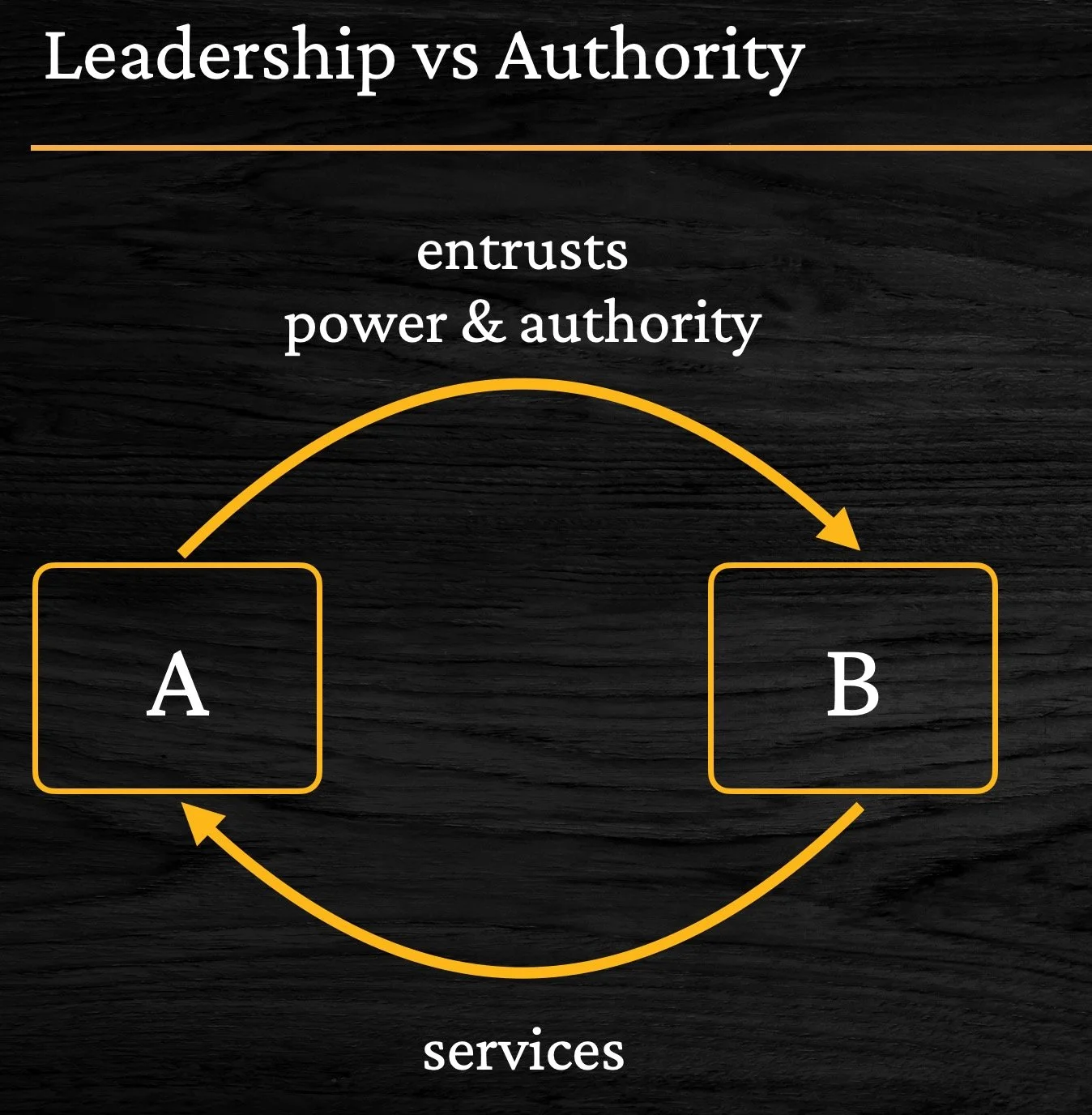
Authority is a role. Leadership is a practice.
Authority performs essential functions. It provides protection, direction, coordination, and management. People depend on it for survival, stability, and continuity. These functions matter deeply in health systems.
But authority does not automatically exercise leadership.
People often look to those in authority hoping they will remove pain, resolve conflict, or deliver certainty. That expectation is understandable. It is also risky. When authority absorbs adaptive work instead of returning it to the system, learning stalls and dependency grows.
Leadership, by contrast, is the practice of keeping the work where it belongs. It helps people face reality, tolerate discomfort, and stay engaged long enough to make progress together.
Exercising leadership often involves disappointing people at a rate they can tolerate, while refusing to collude with avoidance.
Mobilizing collective work
Adaptive leadership is not about individual heroics. It is about mobilizing a collective to work on a shared problem.
That mobilization requires attention to patterns, not personalities. It asks what values are in tension, what losses are being avoided, and how responsibility is being distributed.
This is slow work. It is relational. It often feels inefficient, especially in systems trained to value speed, certainty, and control. Yet without it, organizations repeat the same conflicts with new language and familiar outcomes.
Exercising leadership in health systems and education
I encounter this work daily in clinical settings, in system-level decision making, and in teaching.
As an educator, particularly in undergraduate and professional training, exercising leadership means resisting the urge to deliver clarity too quickly. It means designing learning environments that allow uncertainty to stay visible, questions to remain open, and responsibility to sit with the learner rather than the instructor.
Whether in a classroom, a hospital, or a boardroom, the work is similar. The task is not to have the answer. The task is to hold the question long enough for learning to occur.
Why this work matters
Adaptive leadership is not value-free. It is oriented toward responsibility, learning, and shared ownership of hard problems.
It asks people to stay in relationship when disagreement arises, to examine how power is being used, and to notice what is being protected when change is resisted.
This work is demanding. It cannot be done alone. And it cannot be rushed without cost.
But when it is practiced with care, it creates the conditions for progress that is durable, humane, and worthy of the systems we serve.
What next?
This page is an entry point, not a conclusion. Adaptive leadership is learned over time, through practice, reflection, and shared inquiry. The pages that follow explore the ideas, influences, and teaching approaches that have shaped how I work with these questions, and how I continue to learn alongside others doing this work in complex systems.